A fingerprick test in the ambulance gives the right stroke treatment faster! 🧠🚑 Newcastle University is leading a study across four NHS ambulance services to help paramedics identify severe strokes faster, with the aim of speeding up treatment and improving recovery.
It's called the PRONTO study, btw, and it's investigating new ways to rapidly spot people who've had a large vessel occlusion (LVO) stroke... caused by a blockage in one of the brain's major arteries.
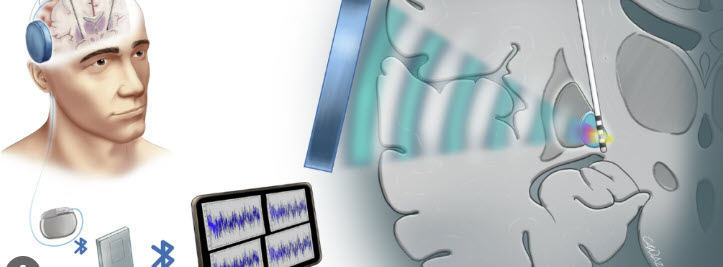
As you most probably know anyway, LVO strokes often require thrombectomy, which removes the clot and restores blood flow to the brain, and the faster it's done, the better the chances of survival and recovery. The trouble is that ambulance crews currently have no reliable test to identify an LVO before they reach hospital. This means thatso many patients first go to a local hospital for assessment, then get transferred on to a specialist centre if a thrombectomy is needed... losing precious time in the process.
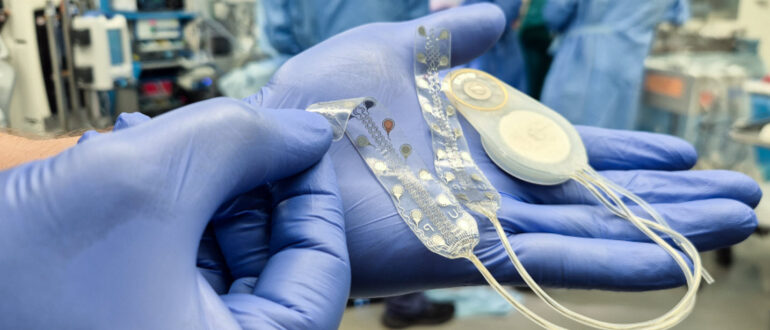
PRONTO combines a simple fingerprick blood test (the LVOne test, developed by Upfront Diagnostics) with direct communication between ambulance crews and hospital specialists. The test measures two blood biomarkers, d-dimer and GFAP, which earlier hospital research suggests can help flag an LVO stroke. Spot the right patients in the ambulance, and they can be taken straight to a centre that can perform the thrombectomy, skipping the delay of assessment at a local hospital first.
Professor Christopher Price, who's co-leading the study with Dr Lisa Shaw, says the hospital results were promising, and that if the study succeeds, the test would speed up treatment and improve recovery for a large number of stroke survivors.
ARNI page followers well know thrombectomy access is one of the biggest bottlenecks in UK stroke care... so fingers cross#ARNIstrokerehabw#stroketreatmentN#thrombectomy##lvostroket#StrokeResearchomy #LVOstroke #StrokeResearch
... See MoreSee Less
What if a tiny chip could actually 'copy' your arteries and predict your stroke risk?! 🧠🔬 Researchers at the University of Sydney and the Heart Research Institute have built an artery-on-a-chip platform that recreates a patient's own carotid artery,. They call it a 'physical twin'; it replicates your specific vascular structure (and the way blood actually flows through it) using cells that behave much as they do in the real thing.
So, why bother? Lead author Lining Arnold Ju explains in Cell Biomaterials yesterday that even patients classed as 'low risk' can suffer severe or fatal strokes, so they wanted a better way to predict who's really in danger. His team reconstructed carotid arteries from six patients with varying degrees of disease, used computational fluid dynamics to map how blood moved through each one, then used a laser to create a small injury and watched what happened.
And the clotting behaviour differed strikingly depending on the shape of the artery. Their conclusion is that the three-dimensional shape of your artery (plus the local flow disturbances within it) are stronger predictors than simple narrowing, which is what current risk assessment mostly relies on... .
Btw, Charles Zhao, moved into stroke prediction research after losing his grandma to a stroke during his PhD time, and he really hopes the tools he's examining will allow drugs to be tested and treatment tailored to each patient's anatomy. The team is now recruiting stroke patients for a clinical trial, and think the same approach could be applied to peripheral artery disease, deep vein thrombosis and aneurysms.
So, if artery shape per se predicts risk better than narrowing does, a lot of people currently told they're 'low risk'#ARNIstrokerehabs#StrokePreventions#StrokeRiske#MedicalResearchk#strokeawarenessb #StrokePrevention #StrokeRisk #MedicalResearch #StrokeAwareness
... See MoreSee Less
Approximately 40% of stroke survivors experience this difficulty: to comprehend or produce spoken or written language caused by a cerebrovascular accident. In half of these cases the language impairment still persists one year post-stroke. Aphasia has wide-ranging effects on the ability to function and quality of life of stroke survivors and easily leads to social isolation.
If you need help, ARNI SLT Telerehab can now help YOU, right now, wherever you are in the world!
The latest evidence shows clearly that you can conquer aphasia very successfully with the help of speech and language therapy.
And it also shows that SLT Telerehab is just as effective as in-person, face to face treatment.
We have a team of highly experienced low-cost specialist SLTs (all post-grads from Universities such as UCL, the University of Cape Town etc) who are available to help you right now, in your home, via Zoom. You get a one to one hourly service, based around your diary needs, from the comfort of your own home, with a highly experienced specialist speech and language therapist. Please enquire to arni.uk.com/get-remote-speech-language-help-now/ !
#aphasia #StrokeSurvivors #strokerecovery #strokerehabilitation #strokerehab #aphasiaawareness #neurorehabilitation #arni #exerciseafterstroke #strokeexercise #strokerecoveryexercises #neuroplasticity #ARNIstrokerehab
www.arni.uk.com
... See MoreSee Less
Petr Piokomy is a qualified specialist personal trainer in stroke and neurological rehabilitation, and has been working in this field for the past 16 years. For the last 7 of those, he's been an associate of the ARNI Institute.
To keep this service running, ARNI relies heavily on donations and a small portion of commission from training sessions. Compared to private neuro rehab centres, ARNI offers a highly affordable and effective alternative - but they need support to keep going.
Here's how Petr is helping:
On Friday, September 25, 2026, ARNI instructor Petr will be taking on 13 Valleys challenge in Lake District in effort to raise awareness and funds for ARNI. This is around 114 miles throughout the national park with over 7,000 metres of elevation gain. This will be the longest and most challenging run he has run and is classed as ''brutal'' difficulty.
This is no small challenge - but it’s nothing compared to what many stroke survivors face every day.
If you can spare anything at all, we'd be be truly grateful for your support. Every donation helps ARNI deliver life-changing rehabilitation to someone who needs it.
www.justgiving.com/page/petr-pokorny-6?utm_medium=FA&utm_source=CL
#exerciseafterstroke #strokeexercise #neurorehab #strokerehabilitation #strokerehab
... See MoreSee Less
A common compensatory strategy after stroke is when someone leans their torso forward to reach something; instead of extending their affected arm fully. They are not always bad and are sometimes needed in order to achieve a task.
Don't let compensatory strategies become the norm for you. Work past them. And if you need some help we have trainers throughout the country who can work with you. Call us on 0203 053 0111 or email support@arni.uk.com to find out if there's one near you.
www.a#strokerecoveryexercisesy#exerciseafterstrokef#neurorehabilitationb#strokerehabilitationb#strokeexercisek#strokerehabt#strokerecoveryk#neuroplasticityp#neurorehabneurorehab
... See MoreSee Less
Stuck in 'fight or flight mode' since your stroke, months on?! There's a reason for it. 🧠 @James Haldane just raised this in our community; he had a large MCA infarct and has been in constant fight or flight mode for six months, with his emotions all over the place.
So, James, your instinct about the amygdala is a good one... the MCA territory supplies the insula, one of the brain's main autonomic control centres; the right insula tends to govern sympathetic tone (the accelerator) and the left the parasympathetic (the brake). And so, damage there disrupts the balance, which is why so many survivors describe feeling permanently 'revved up', with loads of adrenaline.
Right MCA strokes also reduce activity in the anterior cingulate cortex and connected limbic regions, the areas that normally modulate emotional responses; when they're offline, emotions have few filters to regulate them. This is called post-stroke emotionalism, and it affects around one in five survivors at six months, though it tends to decline over the first year, which may give you some comfort buddy...
Btw, for coping, slow-paced breathing has some evidence behind it for shifting autonomic balance and improving heart rate variability, and it can be done anywhere, lying down, in short bursts. CBT has the strongest evidence of any psychological approach and obviously SSRIs are first-line for emotional lability and worth discussing with your GP, since trials show real reductions in emotionalism. Gabapentinoids can work too - although for both those and SSRI's, you must do your homework about side-effects. As back here to the ARNI stroke rehab community @followers if you need... there's lots of experienced people here....
And watch your sensory environment; a noisy, busy room can rally tax your already-taxed nervous system and often its hard to work out what set the reaction off. That's it from me, but good luck with this and take comfort in that James, most survivors find this eases over the first year. 🧠💙
www.arni.co.uk
#ARNIStrokeRehab #PostStrokeEmotionalism #StrokeRecovery #MCAStroke #StrokeSurvivor
... See MoreSee Less
Whenever you’re sitting at a table, it’s a great time to do some hand exercises. You can use various household items like coins, paper clips, silverware or pens to practice a variety of fine motor skills. For example, you can practice gripping a pen, sliding it across the table, and releasing it. Additionally, you can work on using your thumb and fingers to spin the pen in a circle on the table in both clockwise and counterclockwise directions. Practicing tracing and writing can also be effective for improving fine motor coordination skills.
The key is to consistently perform high repetitions of targeted exercises. High repetition is key to recovery because it helps activate neuroplasticity, the mechanism the brain uses to rewire itself and recover.
If you struggle with severe spasticity, which often results in clenched hands after stroke, you can start with passive exercises and stretching. Passive exercise involves assisting your affected hand though a movement, either with the help of a therapist or by using your non-affected hand.
Not sure what you need to do and need some help? Call us on 0203 053 0111 or email support@arni.uk.com and we'll see if there's an instructor near you ,
www.arni.co.uk
#neurorehabilitation #strokeexercise #strokerehabilitation #exerciseafterstroke #neurorehab #neuroplasticity #strokerecovery #strokerecoveryexercises #arnistrokerehab
... See MoreSee Less
Here’s why engaging an ARNI Stroke Rehab UK instructor is a vital step in the stroke recovery journey:
Leveraging Neuroplasticity: ARNI focuses on functional, task-related practice to retrain the brain and body. By engaging survivors in repetitive, meaningful activities, instructors help tap into the brain's neuroplasticity... its ability to reorganise itself to recover lost skills.
Building Functional Independence: ARNI goes beyond passive treatment by teaching practical coping strategies for managing daily life. This includes crucial, real-world tasks like safely getting up from the floor, which builds confidence and functional independence.
Providing Continued, Personalised Support: Unlike standard rehabilitation which can cease once a patient can mobilise, ARNI trainers provide personalised, one-on-one sessions that are constantly adapted and intensified based on the survivor's progress. This bridges the gap in care and combats the risk of a plateau or regression in recovery.
Evidence-Based and Innovative: The ARNI approach incorporates stroke-specific strength and resistance training, which recent research has confirmed improves recovery outcomes. The model challenges the traditional paradigm that recovery plateaus shortly after hospital discharge, offering a framework for enhancing patient outcomes and promoting self-reliance.
Home Retraining: By continuing recovery in a familiar home environment, ARNI also helps reduce stress and anxiety. This empowers survivors to take an active and confident role in their own long-term journey toward regaining strength, balance, and independence.
Call ARNI now on: 0203 053 0111. Don't Delay Do It Today: www.arni.co.uk
#ARNIStrokeRehab #StrokeRecovery #StrokeSurvivor #Neuroplasticity #ARNI
... See MoreSee Less