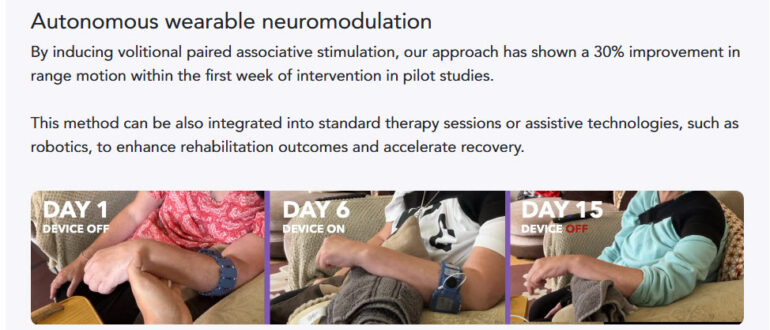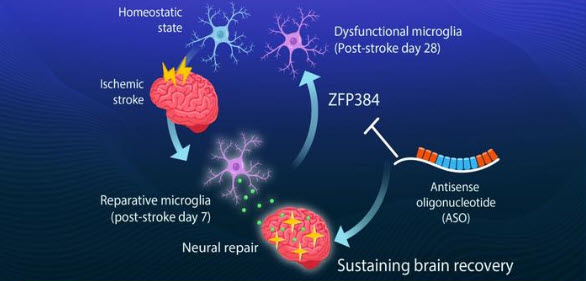
After a stroke, the brain runs a repair programme of its own. The microglia, the brain’s resident immune cells, switch out of their initial inflammatory state and into a reparative one, producing growth factors such as insulin-like growth factor 1 (IGF1) that rebuild myelin around damaged nerve fibres and strengthen synaptic connections. This is a large part of what makes the early months after stroke so productive for rehabilitation… but it only lasts around two months, and once it fades, deficits tend to become permanent. Why it fades has never been well understood…
A team at the Institute of Science Tokyo, working with the Tokyo Metropolitan Institute of Medical Science, Kyushu University and the University of Freiburg, published their findings in Nature on 13 May 2026. They identified a transcription factor called ZFP384 which rises as the microglia lose their reparative properties; it disrupts the chromatin interactions mediated by a protein called YY1 that the microglia need in order to express their repair genes. The point with ZFP384, is that as it climbs, the repair programme switches off regardless of whether the brain still needs it. When the team deleted the Zfp384 gene from microglia in mouse stroke models, those animals held onto their recovery-associated gene expression far longer, with better remyelination, more synaptic plasticity and improved long-term neurological function.
They then built a therapeutic antisense oligonucleotide, ASO-Zfp384, to suppress the gene directly. An ASO is a short synthetic strand of nucleic acid designed to bind to the messenger RNA of a specific gene and trigger its degradation, turning that gene’s expression down. Six ASOs already hold FDA approval across three neurological conditions, including nusinersen for spinal muscular atrophy and tofersen for SOD1-associated ALS. ASOs cannot cross the blood-brain barrier when given systemically, so they are delivered by intrathecal injection into the cerebrospinal fluid, spreading along the neuraxis into the spinal cord and brain; imaging studies show glial cells take them up before neurons do, which matters here, since microglia are the target.
The timing of the ASO-Zfp384 results is significant… the treatment sustained microglial reparative function and still worked when given a week, and even a month, after stroke onset; far outside the window in which clot-busting drugs are useful. Rather than suppressing inflammation, which has been the conventional approach, it retained the brain’s own repair programme. The team then examined brain tissue from human stroke patients and found the same relationship: as the human equivalent, ZNF384, rose, IGF1 declined. This is obviously animal research and the distance to the clinic is considerable; the next stage is safety and efficacy testing in larger preclinical models before any move toward human trials, so realistic NHS availability is a decade or more away. But. very interesting data to absorb.