Chronic pain is one of the most prevalent and least adequately treated sequelae of stroke. Research suggests that approximately 42% of stroke survivors are living with chronic pain six months or more after their stroke… and with around one million stroke survivors in the UK, that points to roughly 420,000 people managing pain as a direct or indirect consequence of their stroke, a number projected to grow substantially as the stroke survivor population is expected to more than double by 2035.
The pain broadly divides into two categories. Central post-stroke pain (CPSP) arises directly from damage to the spinothalamic pathways and thalamic structures involved in pain processing; it’s characterised by burning, aching or hypersensitivity and responds poorly to conventional analgesics. Musculoskeletal pain- including chronic low back pain – arises from the biomechanical consequences of stroke; altered gait, spasticity, pelvic tilt, inhibited core and gluteal muscles, and hours spent in poorly supported positions all drive cumulative mechanical stress into the lower spine over months and years. Lower back pain in particular becomes a significant independent barrier to rehabilitation, reducing exercise tolerance, disrupting sleep and compounding fatigue.
Current treatment options are limited. Opioids carry serious risks of dependence and cognitive blunting, especially concerning in a population already managing potential cognitive impairment. Existing implantable spinal cord stimulators work but require invasive surgery, battery replacement and are expensive… none of which makes them easily accessible to most stroke survivors.
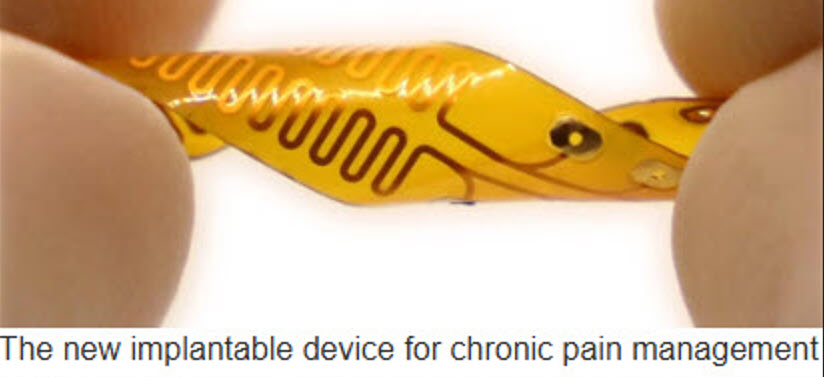
This is why the work from Professor Qifa Zhou at the Zhou Lab, USC Viterbi School of Engineering, published in Nature Electronics in June 2025 and developed in collaboration with the Jun Chen Group at UCLA – deserves attention. Lead author PhD candidate Yushun Zeng and the team have developed a flexible ultrasound-induced wireless implantable (UIWI) stimulator that receives power entirely from a wearable external ultrasound transmitter worn over the skin, with no batteries, no wires and no repeated surgery. The device uses the piezoelectric effect – converting ultrasound mechanical waves into electrical stimulation delivered to the spinal cord – and integrates machine learning algorithms that read physiological signals in real time and adapt stimulation continuously rather than delivering a fixed response. For a stroke survivor whose pain fluctuates with activity, fatigue and spasticity throughout the day, that adaptive capacity is definitely a serious clinical step beyond anything currently available.
Routine clinical use in the UK will be some years away; MHRA licensing and NICE appraisal following human trials would realistically place this five to eight years from now at minimum. But the direction is clear, and that matters. ARNI Stroke Rehab & Recovery says: chronic lower back pain is one of the most consistently reported barriers to rehabilitation that stroke survivors describe to us, and drug-free adaptive pain technology like this represents exactly the kind of progress that could help people keep moving, keep training and keep improving long after their stroke.