This training diary is an essential part of training: no serious stroke survivor who is training with an ARNI Associate can do without these. Order one to start with and you’ll see what we mean.
Designed by Tom Balchin, the way to fill these in is detailed in the Successful Stroke Survivor, and there is a full explanation at the front. Training and the recording of training are equally as important.
... See MoreSee Less
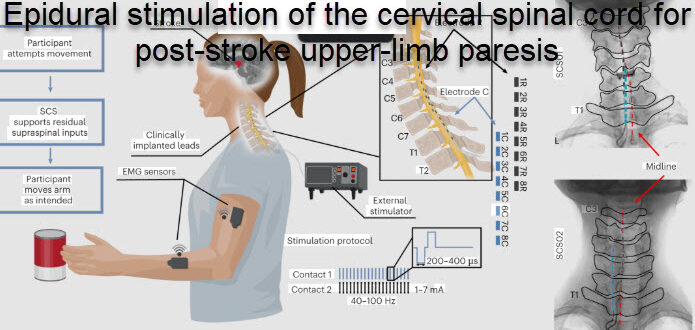
Electrodes in the neck, plus intensive rehab – could this be the best arm stroke recovery combination? 🧠🖐️ A University of Pittsburgh study is now enrolling participants to test pairing cervical epidural spinal cord stimulation with high-dose, high-intensity neurotherapy from MindMaze.
It builds on Pittsburgh's own research, published in Nature Medicine, which showed that stimulating the spinal cord at the neck can improve arm and hand movement in people with chronic stroke after only a few hours of training. But those gains were largely assistive – present while the stimulation was switched on, and gone when it wasn't.
So the new study asks the next question: how much lasting recovery is possible if you deliver that same stimulation alongside serious volumes of therapy? The logic rests on how the nervous system relearns movement; the stimulation creates activity in the spinal cord, your own intent to move pairs with it, and together they strengthen the weakened connections driving the muscles.
What the study wants to know is whether doing that thousands of times over, rather than for a few hours, produces change that lasts once the stimulator is off. Interesting eh? It should do...
MindMaze's platform combines FDA-cleared wearable sensors, motion tracking and AI-driven software to deliver that intensity of active, intent-driven practice without adding to the clinical staffing burden.
The study (NCT07153536) enrols 20 adults with chronic upper limb weakness; participants first complete six weeks of training, then have the stimulation system implanted and repeat the same training with stimulation active throughout, followed for up to six months to see what's retained.
As you know, (potential) recovery after stroke depends largely on (rehab) dosage and intensity. And this study puts that principle at the centre of the design. It's US-based and early at the moment, with only 20 participants, so we'll be watching what the six-month follo#ARNIstrokerehabw#StrokeRecoveryR#UpperLimbRehabS#spinalcordstimulationm#StrokeResearchordStimulation #StrokeResearch
... See MoreSee Less
Do bear in mind Arni has a range of videos available that will guide and assist you with your recovery. Available via online streaming means you can access them from anywhere.
Have you tried them? what did you think????
www.strokesolutions.co.uk/product-category/dvds-and-anytime-viewing/
#ARNIstrokerehab #strokerehabilitation #ARNIstrokerehab #neuroplasticity #arnistroke #strokeexercise #neurorehab #StrokeRecovery #arnistrokecharity
... See MoreSee Less
What if we could extend the brain's own repair window after stroke?! 🧠
We all know about the 'therapeutic time window' and its propensity to fade within over time - which makes it harder to change problems like spasticity and flaccidity...
ARNI has just hard about researchers at the Institute of Science Tokyo who have published a study in Nature identifying why that window closes, and a possible way to hold it open... very interesting reading!
After a stroke, the brain's immune cells (microglia) switch into a reparative state, producing growth factors like IGF1 that rebuild the myelin sheath around nerve fibres and strengthen neural connections... but this only lasts around two months.
The team found that a transcription factor called ZFP384 rises as that repair function declines, switching off the genes the microglia need to keep repairing. So they developed an antisense oligonucleotide (ASO) therapy to suppress it.
And they've found that in mouse models it kept the microglia in their reparative state far longer, improving remyelination, synaptic plasticity and long-term neurological function.
The treatment still worked when given a week, and even a month, after the stroke, well beyond the usual acute window. When the team examined human stroke brain tissue, the same molecular pattern was present, so the mechanism appears to carry over to people.
The idea is to preserve and prolong the brain's own repair programme rather than replace damaged tissue. ARNI Stroke Rehab & Recovery says: survivors are often told by many experts they meet after having a stroke the brain repairs best for a few months after a stroke and then it gradually 'closes' until it's shut - which is of course very far from the truth,...
ARNI Stroke Rehab & Recovery says: an approach that extends the brain's natural recovery window could change what's achievable for the many survivors told their progress had plateaued in the months and years of rehab after stroke.
www.arni.co.uk
#ARNIStrokeRehab #StrokeRecovery #Neuroplasticity #BrainRepair #StrokeResearch
... See MoreSee Less
This is an article written by ARNI Director Tom Balchin. It's from a few years ago but still relevant today so worth re-sharing.
... See MoreSee Less
The Successful Stroke Survivor Volume 3: 47 minutes anytime online viewing
In this exercise video Dr Tom takes you into the realms of serious gait control. Learn how to cope with balance challenges whilst static and moving and learn strategies to combat walking compensations. Tom shows you how to cope with the effects of drop-foot so well that you can look like any non-stroke survivor as you walk down the street. He shows you how to turn smoothly without falling and shows you real-life emergency action control techniques to make yourself confident and safe now that you have removed the need for using a walking stick. Then you get to understand how to cope with steps and slopes… to walk again with surety and control.
www.strokesolutions.co.uk/product/successful-stroke-survivor-dvd-volume-4/
#neurorehab #strokeexercise #strokerehabilitation #ARNIstrokerehab #arnistroke #arnistrokecharity #ARNIstrokerehab #StrokeRecovery #neuroplasticity #stroke
... See MoreSee Less
Repeated attempts to use your affected limbs in training creates a form of practice that can potentially lead to further improvement in performance.
Not sure what to do? Call us on 0203 053 0111 or email support@arni.uk.com to find out if there's a trainer near you who can help you.
www.arni.co#ARNIstrokerehabr#arnistroket#StrokeRecoveryo#arnistrokecharitya#neuroplasticityi#strokerehabilitationa#ARNIstrokerehabr#neurorehabrehab
... See MoreSee Less