Virtual reality (VR) basically means interactive simulations of activities within environments that appear and feel similar to real-world objects and events (augmented reality).
Virtual reality (VR) basically means interactive simulations of activities within environments that appear and feel similar to real-world objects and events (augmented reality).
Would you like to apply (or forward this email to a colleague/friend to consider applying) to come on 15th December 2023 to the VSimulators at Exeter Science Park:
- to get involved with testing cutting-edge VR?
- to take advantage of follow-on exercise of the University lending you prototype VR kit for use at home for 6 weeks?
- to meet Professor Helen Dawes, Dr Tom Balchin & research colleagues & to take part in various workshops?
If so, please read below!
After stroke, survivors who wish to try such augments can find numerous task-training systems on the market that involve a variety of activity-based games that test and (purport hopefully to improve facets of) strength, speed, endurance, range of motion, coordination, timing and cognition.
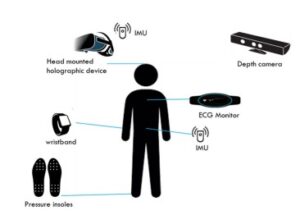
 VR interventions can be expensive but most are usually created to be affordable. A set-up often features just a keyboard, a mouse, a specialised multi-modal device such as a console or gloves with built-in movement sensors. Haptic devices are a good example of this. VR devices often provide feedback on movement execution and goal attainment. Many will help you to repetitively practice large and small movement-based tasks through the use of fun and motivating activities that can be completed while sitting, standing or lying.
VR interventions can be expensive but most are usually created to be affordable. A set-up often features just a keyboard, a mouse, a specialised multi-modal device such as a console or gloves with built-in movement sensors. Haptic devices are a good example of this. VR devices often provide feedback on movement execution and goal attainment. Many will help you to repetitively practice large and small movement-based tasks through the use of fun and motivating activities that can be completed while sitting, standing or lying.
Upper-limb VR kit is popular at the moment because many users report positive changes in fine manual dexterity, grip force, and motor control of their more-affected upper limbs. You may therefore find that it integrates with your current rehabilitation if you can find a suitable device.
 A meta-analysis conducted in 2020 reports a comprehensive search investigate the efficacy of virtual reality (VR) and gaming-based interventions for improving upper extremity function post-stroke, and to examine demographic and treatment-related factors that may moderate treatment response, conducted within the PubMed, CINAHL/EBSCO, SCOPUS, Ovid MEDLINE and EMBASE databases for articles published between 2005 and 2019. This analysis revealed that on average, VR or gaming interventions produced an improvement of 28.5% of the maximal possible improvement.
A meta-analysis conducted in 2020 reports a comprehensive search investigate the efficacy of virtual reality (VR) and gaming-based interventions for improving upper extremity function post-stroke, and to examine demographic and treatment-related factors that may moderate treatment response, conducted within the PubMed, CINAHL/EBSCO, SCOPUS, Ovid MEDLINE and EMBASE databases for articles published between 2005 and 2019. This analysis revealed that on average, VR or gaming interventions produced an improvement of 28.5% of the maximal possible improvement.
Of particular significance: dose and severity of motor impairment did not significantly influence rehabilitation outcomes. Treatment gains were significantly larger overall (10.8%) when the computerized training involved a gaming component vs just visual feedback. VR or gaming interventions showed a significant treatment advantage (10.4%) over active control treatments.

ARNI Stroke Rehab and Exeter University invite you to test examples of upper-limb VR kit on 15th December 2023 (10:00 – 17:00) in the world-class VSimulators building at Exeter Science Park, plus a follow-on exercise of lending you VR kit to for use at home for 6 weeks.
Would you personally like/are you able to apply get involved? Please apply now if appropriate, to come along and get involved in this super opportunity…
The day will be split into two Sections:
- Section A is Workshop entitled: ‘Stroke Rehab Principles: The Strategies & The Evidence’ led by Dr Tom Balchin, Director of The ARNI Institute, where you will learn about cutting edge rehabilitation techniques for people who have had stroke. You will also have the chance to ask Tom all the questions you’ve ever had about rehabilitation after stroke.
- Section B is a VR Research Section led by researchers from University of Exeter Medical School, including Professor Helen Dawes, Professor of Clinical Rehabilitation. You will have chance to try out our special virtual simulator laboratory and try different games for upper limb and balance rehabilitation. You will also be introduced to a new tele-rehabilitation device which you will be able to use in your own home as part of a 6-week study. Lunch will be provided in-between sessions.

Research Session 1: you will take part in a study that give you the chance to try five game-based exercise platforms that can detect your movements using laptop and webcam. Each game consists of several activities designed to train your upper limb and trunk control from a sitting or standing position, according to your abilities.
In this session, you would do some exercises for your upper limbs from seated or standing positions to determine how well you can do the exercises and if these games will be helpful as home-based exercise for people who have had a stroke.
The research team will also ask you about your expectations (before the testing), your experience, and how you found the exercises (after each game).

Research Session 2: you will be invited to try a home-based, immersive reality rehabilitation system, which is designed to detect ‘compensatory’ movement patterns and help you correct them.
Often after stroke people develop compensatory movement patterns in their upper limbs. This system uses an in-built camera to project the user onto their television screen so they can see themselves as an ‘avatar’ as they complete games and exercises. This system is able to track your movement patterns and alert you when you compensate during an activity.
After the Sessions: After the session, you may be able to continue with the study from you own home. Researchers from University of Exeter would help get the RehabKit set up in your home and provide you with personalised upper limb rehabilitation exercises for 6+ weeks.
To register: please get ticket at:
https://www.eventbrite.co.uk/e/758796359337?aff=oddtdtcreator
Or email: movewell@exeter.ac.uk and Exeter University will book you on your behalf.
Email tom@arni.uk.com for inclusion too, plus any questions.


 Another
Another  The analysis was limited in many ways: for example. the highest number of studies conducted to date have been in Asia, Europe, and North America, and no studies have been reported from Africa, South America, and Australia, so this problem adversely affected the generalisability of the study results. Nevertheless, the results of this large-scale meta-analysis show that, compared to the elderly who did not receive the flu vaccine,
The analysis was limited in many ways: for example. the highest number of studies conducted to date have been in Asia, Europe, and North America, and no studies have been reported from Africa, South America, and Australia, so this problem adversely affected the generalisability of the study results. Nevertheless, the results of this large-scale meta-analysis show that, compared to the elderly who did not receive the flu vaccine,

 The Department of Computing at Imperial College London is evaluating a platform called ‘CogiGames Home’, and have asked ARNI Charity to pass this message below to stroke survivors, carers (and professionals to forward if appropriate):
The Department of Computing at Imperial College London is evaluating a platform called ‘CogiGames Home’, and have asked ARNI Charity to pass this message below to stroke survivors, carers (and professionals to forward if appropriate): 




 Balance (both standing and walking) training is the only effective treatment for balance disorders, as recommended by the National Institute for Health and Care Excellence (NICE) UK
Balance (both standing and walking) training is the only effective treatment for balance disorders, as recommended by the National Institute for Health and Care Excellence (NICE) UK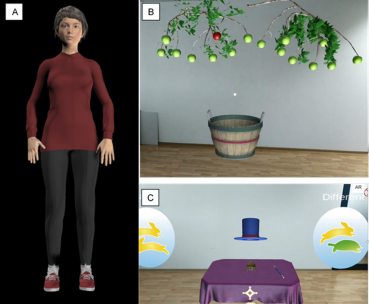 At University College London’s Institute of Neurology, a large-scale global research project (funded by a European Union Horizon 2021 grant), is under way (led by
At University College London’s Institute of Neurology, a large-scale global research project (funded by a European Union Horizon 2021 grant), is under way (led by 
 First, a member of the research team will contact you and see if you are eligible. This will involve them asking you some questions to make sure you are:
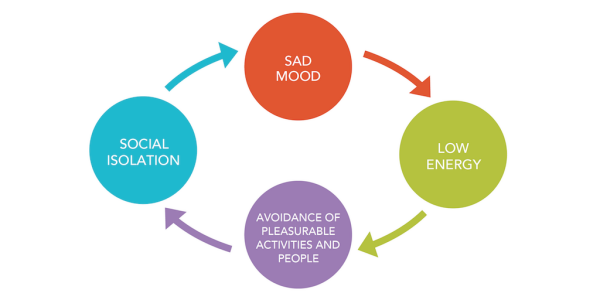
First, a member of the research team will contact you and see if you are eligible. This will involve them asking you some questions to make sure you are: For further help with this issue, please contact DEPRESSION ALLIANCE: A UK charity which helps people with depression, run by sufferers themselves.
For further help with this issue, please contact DEPRESSION ALLIANCE: A UK charity which helps people with depression, run by sufferers themselves. 
 The new (April 2023) stroke guidelines state (click link):
The new (April 2023) stroke guidelines state (click link):  However, access to specialist balance rehabilitation services can be poor due to the lack of enough specialists and sufficient health resources. Current programmes can be sub-optimal in that they are not truly multisensory, do not include any cognitive component (which is a key factor in determining both static and dynamic balance), and do not address real life symptoms reported by patients as challenging.
However, access to specialist balance rehabilitation services can be poor due to the lack of enough specialists and sufficient health resources. Current programmes can be sub-optimal in that they are not truly multisensory, do not include any cognitive component (which is a key factor in determining both static and dynamic balance), and do not address real life symptoms reported by patients as challenging.
 Research, led by
Research, led by 


 During the focus group, the team will have you watch a video which explains the HOLOBalance system. The team will then conduct semi-structured interviews related to the system usability and experience. They may also ask you additional questions as a group, to gather further feedback on the system.
During the focus group, the team will have you watch a video which explains the HOLOBalance system. The team will then conduct semi-structured interviews related to the system usability and experience. They may also ask you additional questions as a group, to gather further feedback on the system. 


 So many stroke survivors, at varying points during their respective times from stroke, have no idea how to start (or re-start) their recoveries. Or they do know about some options. But in either circumstance a majority don’t know what to do for themselves to stand the best chances of gaining some functional success for their efforts.
So many stroke survivors, at varying points during their respective times from stroke, have no idea how to start (or re-start) their recoveries. Or they do know about some options. But in either circumstance a majority don’t know what to do for themselves to stand the best chances of gaining some functional success for their efforts. 
 The reason why it’s important to be able to ‘contextualise/frame yourself’ in terms of the possible progress you can make by comparing yourself to existing data (seeing where you might fit or be one of those outliers etc), is that in the community, it’s very unlikely that you’ll be able to have any of the types of measures applied to you that therapists use clinically on patients unless one is working actively with a therapist.
The reason why it’s important to be able to ‘contextualise/frame yourself’ in terms of the possible progress you can make by comparing yourself to existing data (seeing where you might fit or be one of those outliers etc), is that in the community, it’s very unlikely that you’ll be able to have any of the types of measures applied to you that therapists use clinically on patients unless one is working actively with a therapist. For instance, if you love playing golf and really want to get back to it after stroke, it might not be appropriate to practise straightaway with your Number 5 iron in your house, unless you have a high ceiling and your control is already very good!
For instance, if you love playing golf and really want to get back to it after stroke, it might not be appropriate to practise straightaway with your Number 5 iron in your house, unless you have a high ceiling and your control is already very good! 

 Finding a Speech and Language therapist after discharge is notoriously difficult and SLTs are almost exclusively clinical and/or have big case-loads to take care of. And we know that SLT is often prohibitively expensive to engage with or just unaffordable, meaning people just get incredibly frustrated.
Finding a Speech and Language therapist after discharge is notoriously difficult and SLTs are almost exclusively clinical and/or have big case-loads to take care of. And we know that SLT is often prohibitively expensive to engage with or just unaffordable, meaning people just get incredibly frustrated.
 Storm Anderson, a UK-based speech and language therapist who has predominately treated adults affected by stroke and other acquired brain injury in acute hospital settings as well as out-patient and home-based settings. She has completed her BSc in Speech Language Pathology and MSc in Stroke Medicine, and is currently undertaking her PhD at Queen Square, UCL, using the PLORAS (Predicting Language Outcomes After Stroke) datasets.
Storm Anderson, a UK-based speech and language therapist who has predominately treated adults affected by stroke and other acquired brain injury in acute hospital settings as well as out-patient and home-based settings. She has completed her BSc in Speech Language Pathology and MSc in Stroke Medicine, and is currently undertaking her PhD at Queen Square, UCL, using the PLORAS (Predicting Language Outcomes After Stroke) datasets. Olivia Hodgkinson, a Johannesburg-based qualified Speech Language therapist who completed her BSc and MSc in Speech and Language Pathology at Cape Town University. She has substantial experience in both clinical (acute, sub-acute, specialised rehab and extended units) and educational settings. who has worked within highly diverse settings and within multidisciplinary teams and units. She has led and run therapy departments, supervised and mentored speech therapy university students, developed school based educational assessment programs and support structures for specialised learning units, initiated and implemented training for staff, allied professionals, family and caregivers on a variety of scope related topics in school, hospital and community based settings. She has strong dysphagia experience and skills and is a certified Vital-stim practitioner. She has a great passion for adult neurological injuries and disorders, voice disorders and dysphagia and is looking forward to helping you!
Olivia Hodgkinson, a Johannesburg-based qualified Speech Language therapist who completed her BSc and MSc in Speech and Language Pathology at Cape Town University. She has substantial experience in both clinical (acute, sub-acute, specialised rehab and extended units) and educational settings. who has worked within highly diverse settings and within multidisciplinary teams and units. She has led and run therapy departments, supervised and mentored speech therapy university students, developed school based educational assessment programs and support structures for specialised learning units, initiated and implemented training for staff, allied professionals, family and caregivers on a variety of scope related topics in school, hospital and community based settings. She has strong dysphagia experience and skills and is a certified Vital-stim practitioner. She has a great passion for adult neurological injuries and disorders, voice disorders and dysphagia and is looking forward to helping you!
 Are you a stroke survivor aged 65 years old or older, who has had a stroke at least 6 months ago?
Are you a stroke survivor aged 65 years old or older, who has had a stroke at least 6 months ago?